With a wealth of experience at ICS Medical Devices, we know what it takes to accelerate your product through its development life cycle effectively and efficiently. So let us pass some of that knowledge on to you, and take you through the three most common catheter design mistakes that we’ve seen made, and more importantly – how to avoid them.
Mistake #1
Not deciding what is important to your design; identifying and separating the ‘must–haves‘ and the ‘nice-to–haves’ for your design and deciding what trade-offs you can make.
Firstly, ask what must your catheter be able to do. For example, ‘it must deploy a high radial force stent, which has a deployment force of 25N, with a positioning accuracy of +/-1mm, under fluoroscopy guided imaging, in peripheral arterial vasculature above the knee applications’.
Next, ask what would you like the catheter to do. In our example of a peripheral stent delivery catheter, below the knee access should have an advantage but this may require a different catheter construction (strength and structure, flexibility and profile) that may not be compatible with your priority, which is delivery of the high radial force stent in the above the knee application.
Radial access capability could have a benefit and open up additional uses, but would this impact the business and project priority?
Next ask what the design will not have. For example, the design will not have features like stent retrieval, or the catheter will not require torque, etc. This may appear simple but it does help to define the boundaries in your design requirements to help focus the design on the right areas.
Ambiguity between the ‘must haves’ and the other ‘haves’ debate, or worse the ‘I want it all’ approach, will typically prolong design, muddy your specifications and may yield a product that does not meet any of your goals.
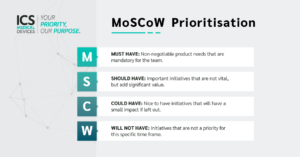
The MoSCoW prioritisation method can be a useful technique in helping you to decide what areas should get the most focus and which should be secondary.
Understanding the priorities and knowing the ‘why’ (i.e. can you justify why you want a particular design or performance in your catheter) is the critical first step in catheter design. This decision will influence how the design cascades into an assembly, sub-assembly and component specifications.
Having a clear understanding your design and its use and user will help to set the priorities and the performances that are up for trade in the prioritisation hierarchy.
Ultimately, setting out the ‘haves’ early can save you time and resources, and avoid confusion later in the development life-cycle.
Mistake #2
Putting your design effort in the wrong place!
Knowledge is a blessing; too much knowledge is often said to be a burden; we believe that knowledge applied in the wrong place is knowledge wasted.
When specifying sub–assemblies and catheters, we apply the fundamentals of Value Engineering – designing and subsequently specifying the features that are important to your device’s functionality and safety. This has double benefit; initially your design efforts are focussed in the right area, and subsequently manufacturing will build the right product.
The Pareto Principle is apt here; 80% of your effort to focus on 20% of your design – the right 20%, the must haves.
Too often there is a rush to apply specifications to every detail in a forensic way, and even good engineers can mistakenly believe it is good practice to apply the highest level of detail and tolerance to every dimensional, functional and material specification, often forgetting to calibrate these with the factors important to their actual design function and the device’s purpose.
Good specification development cascades for the must–haves and focusses on those features.
So, for example, if your catheter shaft is for stent deployment and does carry a load, you should ask:
- What is the load (force) required to deploy that stent? Let’s say 25N from the above ‘must-have’ example.
- Tensile elongation of the shaft is important but not critical, as the positioning accuracy is controlled by a different feature in the design. In this case take 1%.
- What is the force transfer loss through the shaft/system? Take a baseline, in this case take 20%, but this can be reviewed as you generate more data and your test methods help you understand what is happening in your system.
- What factor of safety do you allow? Typically 1.5 times.
Calculate these inputs back into your assembly specification:
25N + 20% loss by 1.5x safety factor = 45N min.
Now that you know your design specification, you can build this back into your catheter construction:
- Composite (reinforced) shaft. Overall wall thickness, OD, ID and profile along overall length.
- Shaft liner (lubricious and durable = typically PTFE).
- Composite wire, sizing, braided pattern optimal for tensile and flexibility.
- Shaft Jacket material and dimensions.
- Radio–opaque markerband / polymer radio-opaque material loading.
- Reinforcement or advantage added to your shaft if required.
Remember – you are not designing for 1:1 torque, nor designing for neurovascular type vasculature and 5mm radius kink capability, and you may not require very tight tolerancing on ID/OD.
Mistake #3
Not engaging with your catheter partner early in the process.
Not talking, or more importantly not collaborating, with your catheter partner at critical stages of the development lifecycle has potential to cause issues further down the line.
Working with an engaged and interested catheter partner can give you significant data and can help to guide you through a successful design, prototype, and manufacturing process, ultimately aiding overall project success.
A good partner can provide:
- Actionable design input. Your catheter design partner should possess a deep understanding of the challenges and opportunities that may present along the way.
- Specification development, smart and efficient specifications and tolerancing input.
- Design for Manufacture input. Think about the long-term success of your project through to its commercial life.
- Supply chain solutions. Manage multiple suppliers and provide additional value to you.
- Prototype solutions (quick turn to custom high quality GLP use).
- Understand your design and evaluate prototypes on your behalf. i.e. Input / Output
- Trust. Discretely share your specification and design in a high–trust environment protecting your information and IP.
At ICS Medical Devices we value the opportunity to engage directly and discretely with our customers and help to triage their specifications. As a development and manufacturing partner it is a win-win synergy. We use our agile processes to help you to achieve an excellent design and we get the opportunity to work on interesting and exciting projects.
Contact us today to speak to one of our engineers and to see how we can be of assistance to your project.